What Is It?
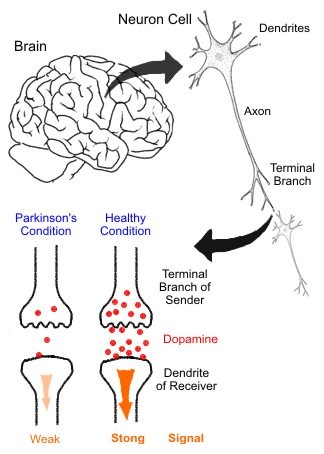
Parkinson's disease is a neurodegenerative disease in which cells in regions of the brain involved with muscular coordination and control suffer in impaired ability to synthesize the neurotransmitter dopamine. Once known as "shaking palsy," it is a disorder of the brain that is characterized by tremors and difficulty with walking, movements, and general coordination. Parkinson disease is named for English physician and geologist James Parkinson (1755-1824). His description of the various manifestations of the disease was published in 1817, in a work entitled "An Essay on the Shaking Palsy." He used the terms "shaking palsy" and "paralysis agitans" to describe a group of related symptoms, which he carefully observed and recorded. It is now known that this neurological disorder is caused by damage to the brain (Gale 2011). The main symptoms of the disease are tremors while at rest and abnormal movements of the arms and legs while standing or walking. These are accompanied by a number of other symptoms, including speech problems, a stiff, bent-over position, insomnia, and constipation. All related disorders are attributed to a malfunction of the basal ganglia (which contain a rich array of neurotransmitters and receptors controlling muscular movements) and of the substantia nigra (where dopamine is produced). Dopamine is one of the brain chemicals involved in the control of physical movement, and Parkinson's disease is characterized by dopamine depletion. Secondary Parkinson's disease, in which symptoms are of a passing nature, is due to temporary dopamine depletion, induced most commonly by antipsychotic drugs.
Description:
Usually beginning in a person’s late fifties or early sixties, Parkinson disease causes a progressive decline in movement control, affecting the ability to control initiation, speed, and smoothness of motion. Symptoms of PD are seen in up to 15% of those ages 65–74, and almost 30% of those ages 75–84. Parkinson's disease affects about 500,000 people in the United States, with approximately 50,000 new cases diagnosed each year. It usually occurs in middle age, typically beginning around age 60. However, about 5% of patients have early onset Parkinson's disease and are younger than 40 years old when symptoms begin (Gale 2010). Internationally, Parkinson's disease affects about 1 to 2 of every 1,000 people. It affects Europeans and North Americans more often than Asians or Africans. It is more common in men than in women.So far, scientists have not determined why some people develop Parkinson's disease and others do not. The genetics are complex and the influence of family history depends on the age when the disease started. A person who has a parent or sibling that was diagnosed with the disease at a younger age is at higher risk of getting Parkinson's, but not if the affected family member was older when diagnosed.
Symptoms:
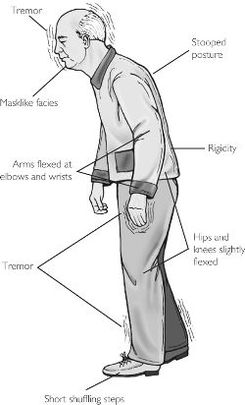
Parkinson's disease usually begins as a slight tremor or stiffness in the arm or leg on one side of the body. The tremor is most obvious at rest and is regular, typically occurring three to six times per second. The Parkinson's disease tremor usually worsens under stress, improves when the arm or leg is moved voluntarily, and may disappear entirely during sleep. In the earliest stages, Parkinson's disease may be evident only as a tremor involving the thumb and index finger. This tremor sometimes is called "pill-rolling" tremor because it looks as if the person is manipulating a small object such as a pill. As the illness worsens, the tremor may become more widespread and eventually affect limbs on both sides of the body. Handwriting may become small, shaky and eventually illegible. In addition to the classic tremor, Parkinson's disease often causes stiffness or rigidity in the muscles of the arms or legs and a slowing of body movements, called bradykinesia (2011). The rigidity and bradykinesia can be the most disabling aspects of the disease. They can impair the person's ability to walk and to do daily activities, such as washing, dressing or using eating utensils. Problems with unsteady balance and posture may make it hard for a person with Parkinson's disease to sit down in a chair or to rise from one. Walking is accomplished with small, shuffling steps and a stooped posture, usually without the normal arm-swinging motions. Bradykinesia can affect the facial muscles, decreasing spontaneous facial expressions and normal eye blinking.The general symptoms of Parkinson's disease include:
Description:
Usually beginning in a person’s late fifties or early sixties, Parkinson disease causes a progressive decline in movement control, affecting the ability to control initiation, speed, and smoothness of motion. Symptoms of PD are seen in up to 15% of those ages 65–74, and almost 30% of those ages 75–84. Parkinson's disease affects about 500,000 people in the United States, with approximately 50,000 new cases diagnosed each year. It usually occurs in middle age, typically beginning around age 60. However, about 5% of patients have early onset Parkinson's disease and are younger than 40 years old when symptoms begin (Gale 2010). Internationally, Parkinson's disease affects about 1 to 2 of every 1,000 people. It affects Europeans and North Americans more often than Asians or Africans. It is more common in men than in women.So far, scientists have not determined why some people develop Parkinson's disease and others do not. The genetics are complex and the influence of family history depends on the age when the disease started. A person who has a parent or sibling that was diagnosed with the disease at a younger age is at higher risk of getting Parkinson's, but not if the affected family member was older when diagnosed.
Symptoms:
Parkinson's disease usually begins as a slight tremor or stiffness in the arm or leg on one side of the body. The tremor is most obvious at rest and is regular, typically occurring three to six times per second. The Parkinson's disease tremor usually worsens under stress, improves when the arm or leg is moved voluntarily, and may disappear entirely during sleep. In the earliest stages, Parkinson's disease may be evident only as a tremor involving the thumb and index finger. This tremor sometimes is called "pill-rolling" tremor because it looks as if the person is manipulating a small object such as a pill. As the illness worsens, the tremor may become more widespread and eventually affect limbs on both sides of the body. Handwriting may become small, shaky and eventually illegible. In addition to the classic tremor, Parkinson's disease often causes stiffness or rigidity in the muscles of the arms or legs and a slowing of body movements, called bradykinesia (2011). The rigidity and bradykinesia can be the most disabling aspects of the disease. They can impair the person's ability to walk and to do daily activities, such as washing, dressing or using eating utensils. Problems with unsteady balance and posture may make it hard for a person with Parkinson's disease to sit down in a chair or to rise from one. Walking is accomplished with small, shuffling steps and a stooped posture, usually without the normal arm-swinging motions. Bradykinesia can affect the facial muscles, decreasing spontaneous facial expressions and normal eye blinking.The general symptoms of Parkinson's disease include:
- Depression
- Anxiety
- Disturbed sleep
- Memory loss
- Slurred or abnormally soft speech
- Difficulty chewing or swallowing
- Constipation
- Impaired bladder control
- Abnormal regulation of body temperature
- Sexual dysfunction
- Cramps, numbness, tingling or pain in the muscles
http://schoolworkhelper.net/parkinson%E2%80%99s-disease-symptoms-inheritance/
What Causes It?
The basal ganglia control movements of the muscles, muscle tone, balance, coordination of groups of muscles that oppose each other, and the change of state necessary for muscles to go from rest to motion. Control from this section of the brain also enables some muscles to remain at rest while others are in action. In a healthy state, signals pass from the motor cortex of the brain to the reticular formation and spinal cord and then to the various muscles that are to undergo contraction. At the same time, other signals follow a different pathway through the basal ganglia, where the nerve signal is dampened (subdued or toned down) so that the resulting contraction does not become jerky (too sudden or quick). Dopamine, found in the basal ganglia, is the neurotransmitter responsible for the dampening effect of the motor signal. If the dampening effect should become too strong, then another neurotransmitter, acetylcholine, counteracts the effects of the dopamine, thus maintaining a balance in the force of the signals sent to the muscle. In Parkinson disease, degeneration of the basal ganglia, along with damage to the dopamine-producing cells of the substantia nigra, hampers the proper functioning of the nerve pathway that controls movements of the muscles. The muscles become excessively tense, a condition that gives rise to tremor and a rigid joint action. The movements of the body also begin to slow down because of this malfunction. Drug treatments are designed to increase the level of dopamine or inhibit the release of acetylcholine, which counteracts dopamine (2011). Damage to the basal ganglia may be caused by an environmental factor, such as an unknown toxic chemical. Another supposition is that an early viral infection causes the degeneration. Parkinson's may follow encephalitis or other forms of brain injury.
Most cases of Parkinson disease probably result from a complex interaction of environmental and genetic factors. These cases are classified as sporadic and occur in people with no apparent history of the disorder in their family. The cause of these sporadic cases remains unclear. Approximately 15 percent of people with Parkinson disease have a family history of this disorder. Familial cases of Parkinson disease can be caused by mutations in the LRRK2, PARK2, PARK7, PINK1 (which plays a role in the cell machinery that breaks down, or degrades, unneeded proteins by tagging damaged and excess proteins with molecules called ubiquitin (GHR 2012)), or SNCA gene, or by alterations in genes that have not been identified. Mutations in some of these genes may also play a role in cases that appear to be sporadic (not inherited).
Most cases of Parkinson disease probably result from a complex interaction of environmental and genetic factors. These cases are classified as sporadic and occur in people with no apparent history of the disorder in their family. The cause of these sporadic cases remains unclear. Approximately 15 percent of people with Parkinson disease have a family history of this disorder. Familial cases of Parkinson disease can be caused by mutations in the LRRK2, PARK2, PARK7, PINK1 (which plays a role in the cell machinery that breaks down, or degrades, unneeded proteins by tagging damaged and excess proteins with molecules called ubiquitin (GHR 2012)), or SNCA gene, or by alterations in genes that have not been identified. Mutations in some of these genes may also play a role in cases that appear to be sporadic (not inherited).
http://dgcbio.wikispaces.com/Parkinson's+Disease
How Do We Fix It?
Treatments:There are organizations that can give families help in learning how to manage the illness in its early stages. Exercise is important along with special aids to help movement. Drug therapy is important in later stages of the disease when symptoms become debilitating if left untreated. The drug treatment is complex because dosages have to be carefully regulated and different combinations of drugs have to be used. For example, despite certain severe side effects, the drug levodopa (L-DOPA) is currently used as the most effective medication in the treatment of Parkinson disease. Some of the adverse side effects are disorders of the digestive system, hemorrhage, disturbances in heart rhythm, depression, confusion, possible psychotic reactions, and delirious episodes (2011). The extent of these reactions appears to be dependent on the amount of medication used. In some patients the mask-like facial expression gives way to distorted facial expressions, and other unusual body movements may result from the use of the drug. A combination drug called Sinemet composed of levodopa and carbidopa (a drug that alleviates levodopa's side effects) is given in careful dosages often requiring changes in the amount taken. Patients respond differently to this combination drug. Some will be able to take it hourly, others just three times daily. Another surgical intervention, widely used in Europe for more than two decades gained U.S. Food and Drug Administration (FDA) in 2002. The procedure involves implanting a pacemaker-like device to provide electrical stimulation to areas of the brain deprived of dopamine. Still more research is being done to find a substance that could potentially prevent the cells within the substantia nigra from dying.
Theoretical Cure:
A controversial area of endeavor associated with PD involves stem cell research. It has been hypothesized that PD could be reversed if appropriate stem cells were transplanted into an affected brain. In particular, it has been suggested that the disease may respond to implantation of dopamine producing neurons derived from stem cells. Animal models are being developed to assess the likelihood and feasibility of this approach. However, medical administration of the missing neurochemical dopamine is ineffective since it apparently does not enter the brain from the blood. Instead, a precursor of dopamine, L-DOPA, is used that can diffuse into the brain where it is converted to dopamine (2010). PD is therefore most commonly treated with pharmaceutical products containing L-DOPA, but in more advanced cases neurosurgical procedures have to be used. With the advent of gene therapy, there is now hope that this will provide a feasible alternative for the long-term treatment of PD. Animal models have shown promising results with the long-term production of L-DOPA following just a single gene therapy treatment. Adeno-associated viral (AAV) vectors have been used to deliver two human genes to the specific area of the brain affected by the disease in PD rat models. There were no observable toxicities after treatment, and importantly, there were no other regions of the brain affected by the gene delivery. Thus, gene therapy may yet prove to be the most effective way of treating PD in the future. Furthermore, dopamine is broken down by several enzyme systems in the brain and elsewhere in the body. Thus, in theory, blocking these enzymes is a key strategy to prolonging the effect of dopamine. The two most commonly prescribed forms of L-DOPA contain a drug to inhibit the amino acid decarboxylase (an AADC inhibitor), one type of enzyme that breaks down dopamine. These combination drugs are Sinemet (L-dopa plus carbidopa) and Madopar (L-dopa plus benzaseride). Controlled-release formulations also aid in prolonging the effective interval of an L-dopa dose (2007).
Theoretical Cure:
A controversial area of endeavor associated with PD involves stem cell research. It has been hypothesized that PD could be reversed if appropriate stem cells were transplanted into an affected brain. In particular, it has been suggested that the disease may respond to implantation of dopamine producing neurons derived from stem cells. Animal models are being developed to assess the likelihood and feasibility of this approach. However, medical administration of the missing neurochemical dopamine is ineffective since it apparently does not enter the brain from the blood. Instead, a precursor of dopamine, L-DOPA, is used that can diffuse into the brain where it is converted to dopamine (2010). PD is therefore most commonly treated with pharmaceutical products containing L-DOPA, but in more advanced cases neurosurgical procedures have to be used. With the advent of gene therapy, there is now hope that this will provide a feasible alternative for the long-term treatment of PD. Animal models have shown promising results with the long-term production of L-DOPA following just a single gene therapy treatment. Adeno-associated viral (AAV) vectors have been used to deliver two human genes to the specific area of the brain affected by the disease in PD rat models. There were no observable toxicities after treatment, and importantly, there were no other regions of the brain affected by the gene delivery. Thus, gene therapy may yet prove to be the most effective way of treating PD in the future. Furthermore, dopamine is broken down by several enzyme systems in the brain and elsewhere in the body. Thus, in theory, blocking these enzymes is a key strategy to prolonging the effect of dopamine. The two most commonly prescribed forms of L-DOPA contain a drug to inhibit the amino acid decarboxylase (an AADC inhibitor), one type of enzyme that breaks down dopamine. These combination drugs are Sinemet (L-dopa plus carbidopa) and Madopar (L-dopa plus benzaseride). Controlled-release formulations also aid in prolonging the effective interval of an L-dopa dose (2007).
